The Great Health Heist: Why Africa Paying Its Own Way Means Western Donors Are Losing Control

The narrative of African self-sufficiency in health funding is a Trojan horse. Unpacking the real power shift and the hidden costs of 'efficiency' in global health.
Key Takeaways
- •The shift to African self-funding risks prioritizing measurable 'efficiency' over equitable access to primary care.
- •Dependency on donors is being replaced by dependency on global financial compliance standards.
- •Expect increased privatization of health services as governments seek efficient revenue generation.
- •The real danger is the widening gap between the health outcomes of the urban rich and the rural poor.
The Illusion of Independence: Who Truly Wins When Africa Pays?
The current clamor around **African health financing**—the idea that the continent can finally fund its own healthcare systems—sounds like a triumph of sovereignty. It’s a feel-good story for Western aid agencies and a necessary political talking point for African leaders. But peel back the veneer of self-reliance, and you find a far more cynical reality. This isn't just about budgetary allocations; it’s about the ruthless prioritization of efficiency over equity, a shift that benefits global finance structures far more than the marginalized populations needing care.
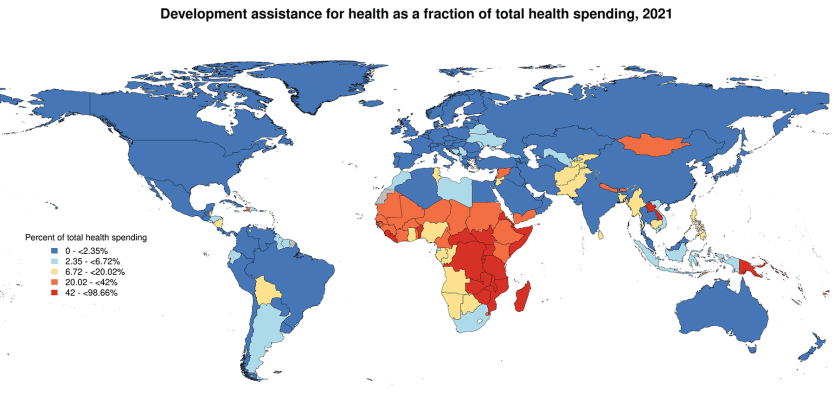
The argument, often championed by entities like the World Bank, centers on redirecting domestic resources—taxes, user fees, and domestic bonds—to plug the massive funding gaps currently filled by external donors. While eliminating dependency on volatile foreign aid seems laudable, the unspoken truth is this: dependency is leverage. When donors pull back, they don't just lose influence; they force African nations into adopting specific, often Western-defined, metrics of ‘efficiency’ that frequently sideline primary, preventative care in favor of high-visibility, measurable interventions.
The Efficiency Trap: A Cost-Benefit Analysis of Human Life
We must analyze the shift toward **global health security** funding through a sharp, contrarian lens. Efficiency in this context rarely means better access for the rural poor; it means optimizing budgets for maximum statistical return on investment (ROI). This drives investment toward urban centers, specialized disease control (like HIV/AIDS or Malaria programs that attract earmarked donor funds), and away from strengthening brittle, underfunded infrastructure like maternity wards or rural clinics. The result? A two-tiered health system where the newly empowered national budget services the politically vocal middle class, while the truly vulnerable are left behind, victims of optimized neglect.
Furthermore, the push for domestic financing often comes with strings attached: fiscal discipline, privatization of certain services, and adherence to international procurement standards. This isn't true financial autonomy; it’s the rebranding of financial control. African nations are trading grant dependency for debt dependency or compliance dependency, all under the banner of 'owning their agenda.' This transition is less about health equity and more about aligning African fiscal policy with global market dictates. The real winners are the external financial institutions setting the new rules of engagement for **public health spending**.
What Happens Next: The Inevitable Privatization Wave
The trajectory is clear. As governments are forced to generate more internal revenue for health, the path of least political resistance will be user fees and public-private partnerships (PPPs). Expect a surge in the privatization of diagnostics, pharmaceuticals supply chains, and specialized hospital management within the next five years across key African economies. This will undeniably increase the *quality* of care available, but only for those who can afford the premium. The gap between the health outcomes of the urban elite and the rural majority will widen dramatically, creating internal social instability that current health metrics fail to capture.
The next great fight won't be for more aid money; it will be for regulatory frameworks that prevent the 'efficient' market from cannibalizing the basic right to health for the poorest citizens. Africa can pay, yes, but the critical question is: Who will be paying, and what* will they be paying for?*
Gallery




Frequently Asked Questions
What is the primary criticism of African nations paying for their own health?
The primary criticism is that the push for 'efficiency' often forces governments to prioritize high-ROI interventions favored by international metrics, neglecting essential, but less measurable, primary and preventative care for the most vulnerable populations.
How does donor dependency differ from compliance dependency?
Donor dependency relies on grants and external funding decisions. Compliance dependency occurs when a nation must adhere strictly to the fiscal rules and procurement standards set by international financial bodies (like the IMF or World Bank) to secure domestic financing mechanisms, effectively trading one form of external control for another.
What is predicted to happen to healthcare access in the near future?
It is predicted that there will be a significant rise in user fees and public-private partnerships, leading to a two-tiered health system where high-quality care becomes increasingly accessible only to those who can afford private or subsidized services.
What is 'global health security' funding?
Global health security funding refers to international investments aimed at preventing, detecting, and responding to infectious disease threats worldwide. While crucial, critics argue it often receives disproportionate funding compared to foundational primary healthcare systems.
